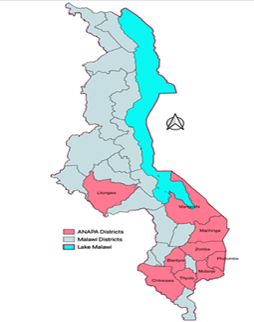
Project HOPE Namibia (PHN), a member of the Africa Public Health Network (APHN), implements a project called Ana ndi Achinyamata Patsogolo Activity (ANAPA) – Children and Youth First, funded by USG in Malawi. The project is implemented in 9 high HIV burden districts of Blantyre, Chikwawa, Lilongwe, Machinga, Mangochi, Mulanje, Phalombe, Thyolo, and Zomba.
By the end of FY25, APHN supported communities within the catchment areas of 142 health facilities, including five Centers of Excellence and multiple government-led sites, reaching 55,862 program participants (children living with HIV (CLHIV), HIV-exposed infants (HEI), and caregivers) with lifesaving facility and community HIV care and treatment services. Among the 10,420 CLHIV enrolled in ANAPA, 99% were eligible and received a viral load (VL) test, and 77% achieved viral suppression by the end of FY25 (compared to 61% at the end of FY24), despite the intentional enrolment of CALHIV with high baseline VL.